
WHEN IT COMES TO PUBLIC HEALTH, policy-makers bear the responsibility of making a wide range of decisions on matters that could be life or death, immediate or far-reaching. Ensuring that their populations have access to quality health services and that there is a sufficient supply of health workers, medicines and technologies requires strong planning based on the latest and best available evidence.
Faced with making quick decisions, policy-makers might rely on their own experiences and intuition. Their world view might inform the approach they take. There might be pressure from their constituents, from lobbyists and from campaigning organizations. And, they might be guided by solid research evidence – but only when there are strong connections between the research and policy-making communities.
Bringing public health researchers and policy-makers together to forge stronger ties and build mutual trust was the motivating force behind the Alliance for Health Policy and Systems Research’s ‘Embedding Rapid Reviews in Health Systems Decision-Making’ (ERA) project.
In 2018 the Alliance started working with researchers in Georgia, India, Malaysia and Zimbabwe to see what difference it would make to have a team of trained and trusted researchers that government staff could rely on for quick answers.
The teams were trained to synthesize evidence from multiple sources and studies to understand what the body of evidence says about a particular topic. But in the interest of working with policy-makers facing tight timelines, they sped up this systematic review process so that the researchers could provide rapid answers for policy-makers.
This process is called rapid review, and just like other evidence synthesis techniques, it comprise four stages:

HOWEVER, AS COVID-19 BECAME a public health emergency and then a pandemic, decision-makers not only needed the best current evidence available, they now needed it at a speed that was previously unheard of.
Here are the stories of how teams in Georgia and India took on that challenge.
GEORGIA

AS PUBLIC HEALTH RESEARCHER, LELA SULABERIDZE, watched a new, deadly virus sweep the globe in early 2020, she feared for her country. She knew that decision-makers in Georgia would have to act fast to save lives.
From her previous work gathering evidence at the ministry of health, she knew that staff there lacked the means to respond quickly to a pandemic and to deal with a potential explosion of cases.
But, as part of a small, crack team of researchers trained in rapid research response, Sulaberidze also knew that she and her colleagues at Curatio International Foundation (CIF) could help.
In early March, when Georgia had recorded its first death from COVID-19, the team at CIF emailed Tamar Gabunia, Georgia’s deputy health minister, offering their services.


She needed instant answers based on solid evidence. The stakes for policy-makers were “very high and very heavy,” and acting on instinct alone could endanger lives, said Gabunia.
The researchers immediately got to work.



THE ERA PROJECT MANAGER Maia Uchaneishvili, divided the CIF team by tasks and location, with two researchers working from home and two from the office.
A report like this would normally take six weeks, but the team knew they’d need to deliver results in a fraction of that time.
They had just seven days to produce a report that would underpin the Georgian government’s response to COVID-19.
THE ERA PROJECT MANAGER Maia Uchaneishvili, divided the CIF team by tasks and location, with two researchers working from home and two from the office.
A report like this would normally take six weeks, but the team knew they’d need to deliver results in a fraction of that time.
They had just seven days to produce a report that would underpin the Georgian government’s response to COVID-19.
THE TASK WAS EXCITING BUT DAUNTING. The researchers didn’t just need to find examples of countries that had successfully dealt with the early stages of the epidemic – they needed to show how they flattened the curve.
Knowing that, if the virus was not quickly contained it could overwhelm Georgia’s health care system, the researchers operated like frontline workers in an emergency.


Limiting their search to Asian countries that had effectively managed COVID-19, they shunned sleep in order to keep scanning for expert analysis and data.
They looked specifically for information about hospital and emergency service capacity, ventilator numbers, testing methods and distancing measures.
They quickly hit a wall trying to find information about COVID-19 from the usual sources, so widened their search to include any and all reports that mentioned these issues. This included finding reports in other languages, even though it meant using precious time in translating them.
George Gotsadze, CIF’s Executive Director, and Senior Researcher, Ivdity Chikovani, worked around the clock at the office and remotely to develop models that showed the potential outcomes and caseloads based on the timing and strictness of distancing measures.
THE TASK WAS EXCITING BUT DAUNTING. The researchers didn’t just need to find examples of countries that had successfully dealt with the early stages of the epidemic – they needed to show how they flattened the curve.
Knowing that, if the virus was not quickly contained it could overwhelm Georgia’s health care system, the researchers operated like frontline workers in an emergency.


Limiting their search to Asian countries that had effectively managed COVID-19, they shunned sleep in order to keep scanning for expert analysis and data.
They looked specifically for information about hospital and emergency service capacity, ventilator numbers, testing methods and distancing measures.
They quickly hit a wall trying to find information about COVID-19 from the usual sources, so widened their search to include any and all reports that mentioned these issues. This included finding reports in other languages, even though it meant using precious time in translating them.

George Gotsadze, CIF’s Executive Director, and Senior Researcher, Ivdity Chikovani, worked around the clock at the office and remotely to develop models that showed the potential outcomes and caseloads based on the timing and strictness of distancing measures.





AS SOON AS THE FIRST draft was ready, Gotsadze hand-delivered it at 23:00 to the Prime Minister’s office. At 10:00 the next morning he and senior CIF colleagues were in the Prime Minister’s office discussing its findings in detail.


Days later, once the final report had gone to the ministry of health and gone public, the researchers saw their evidence, graphs and recommendations popping up everywhere.
AS SOON AS THE FIRST draft was ready, Gotsadze hand-delivered it at 23:00 to the Prime Minister’s office. At 10:00 the next morning he and senior CIF colleagues were in the Prime Minister’s office discussing its findings in detail.

Days later, once the final report had gone to the ministry of health and gone public, the researchers saw their evidence, graphs and recommendations popping up everywhere.
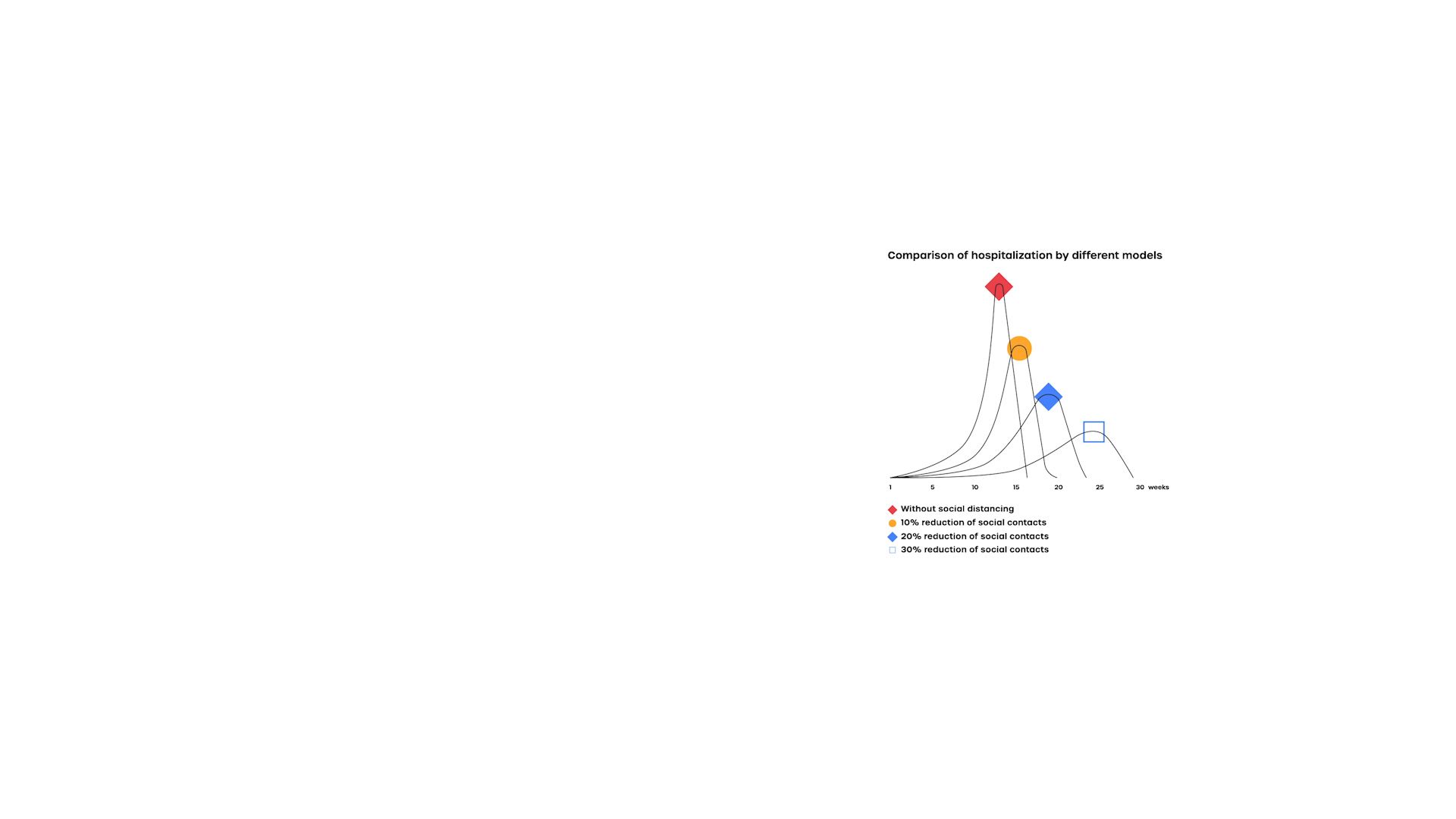

THE MODELLING SHOWING POTENTIAL EFFECTS of different social distancing measures went viral, as people shared and discussed the startling graph comparisons on social media. Media requests for CIF staff poured in, but they could only respond to a limited number as they were busy working on evolving policy measures.


In those early days of the pandemic, CIF worked hand in hand with the government, providing relevant answers to their urgent questions. Embedding the role of research in government policy in this way meant that CIF would play a major role in the Georgian COVID-19 response.
Gotsadze says that the ERA project had built trust between researchers and decision-makers in Georgia so that, when this crisis occurred, they already knew how to work together effectively.
Tamar Gabunia says CIF’s COVID-19 work “played a huge role” in Georgia recording only 735 confirmed cases and 12 deaths [as of 27 May], and that they were providing ongoing help as the government eased restrictions and reopened the economy and borders.
Georgia has been praised at home and internationally for its response to the pandemic and was one of the first to start inviting tourists back.
THE MODELLING SHOWING POTENTIAL EFFECTS of different social distancing measures went viral, as people shared and discussed the startling graph comparisons on social media. Media requests for CIF staff poured in, but they could only respond to a limited number as they were busy working on evolving policy measures.
In those early days of the pandemic, CIF worked hand in hand with the government, providing relevant answers to their urgent questions. Embedding the role of research in government policy in this way meant that CIF would play a major role in the Georgian COVID-19 response.

Gotsadze says that the ERA project had built trust between researchers and decision-makers in Georgia so that, when this crisis occurred, they already knew how to work together effectively.
Tamar Gabunia says CIF’s COVID-19 work “played a huge role” in Georgia recording only 735 confirmed cases and 12 deaths [as of 27 May], and that they were providing ongoing help as the government eased restrictions and reopened the economy and borders.
Georgia has been praised at home and internationally for its response to the pandemic and was one of the first to start inviting tourists back.
FOR CIF'S RESEARCHERS, USING THEIR skills to serve their country and help avoid a public health disaster has been a point of pride and a career highlight.
It developed the skills and confidence, especially of more junior staff, to be able to have more of a back-and-forth relationship with policy-makers, however senior, who relied heavily on their work.

Demand for rapid reviews has increased “drastically over the last two or three months,” said Gabunia.
She expects that will continue over the coming months, but also beyond COVID-19 to help fix any weaknesses in Georgia’s health care system that the pandemic has exposed.
INDIA

PUBLIC HEALTH RESEARCHER SOUMYADEEP BHAUMIK never thought he would be emailing his colleagues late on a Friday to ask them to work with him over the weekend in a virtual command centre he dubbed ‘The War Room’.
But on 19 March 2020, as India was seeing its first reported cases of COVID-19, the government had contacted researchers at The George Institute for Global Health in New Delhi, asking for help to find out how to protect India’s most at-risk frontline health workers – and the vulnerable communities they serve – from catching and spreading the virus.
It was vital to protect the roughly one million community health workers in India, and the countless clients they would meet going door to door in villages, who were largely unaware of this new virus. But it was also key to ensure these so-called Accredited Social Health Activists (ASHAs), who form the backbone of India’s primary health care system, could keep functioning to provide crucial and important services unrelated to COVID-19.


The government needed to know what roles community health workers had played in previous pandemics, and what to equip them with in terms of training, information and equipment.
They also needed evidence-based recommendations to produce written guidelines detailing best practices and potential hazards for the ASHAs – and all within three days.
The researchers were used to working on rapid reviews and evidence synthesis projects that took six to eight weeks; this needed to be done in a fraction of the time. They quickly divided the tasks among the team and began work that same evening. They were separated by home-working, and Bhaumik was stuck in Australia. United by email, Skype and WhatsApp, however, the team was operating almost 24 hours a day.



BHAUMIK AND HIS COLLEAGUE SANDEEP MOOLA spent Friday scanning databases to find evidence from studies, which they screened and analysed.
Misimi Kakoti, who had only joined the organization a month before, and Jyoti Tyagi, searched different governments’ websites for information on COVID-19.
Their teamwork and methods were solid, but they hit plenty of hurdles.
They found a dearth of literature on COVID-19, and key documents were written in French. They widened their search to pandemics within the last two decades, while another colleague, Devaki Nambiar, took time away from maternity leave to help with translations.
BHAUMIK AND HIS COLLEAGUE SANDEEP MOOLA spent Friday scanning databases to find evidence from studies, which they screened and analysed. Misimi Kakoti, who had only joined the organization a month before, and Jyoti Tyagi, searched different governments’ websites for information on COVID-19.
Their teamwork and methods were solid, but they hit plenty of hurdles.
They found a dearth of literature on COVID-19, and key documents were written in French. They widened their search to pandemics within the last two decades, while another colleague, Devaki Nambiar, took time away from maternity leave to help with translations.
AS THE WEEKEND WORE ON, they struggled with exhaustion, but with each new vital discovery they were compelled to keep working. They knew that it fell to them to uncover information that would ensure the right policy choices were made. Ultimately people’s lives were at stake.
By Saturday evening, they had uncovered enough evidence about the experiences of community health workers during other pandemics to provide clear guidelines on how they should work and, crucially, what additional services they should maintain to protect lives in other areas.
By Sunday night, they were able to show that ASHAs would need personal protective equipment, soap and sanitizer and training on myth-busting and misinformation around dangerous virus cures and prevention methods.
Their evidence also showed that frontline workers might face stigma and violence, especially if involved in contact tracing, and might need psycho-social support and should avoid working alone.
On Monday morning, having written all this up, they were able to submit the report. They were relieved, but also anxious. Limited time to check the documents and limited sleep could have meant mistakes.
But Rajani Ved, Executive Director of India’s National Health Systems Resource Centre, which advises state and national governments, says that policy-makers greatly appreciated having evidence and recommendations delivered together.
“If we didn't have the evidence, probably we would have got some of our facts wrong,” she said. The report pointed the government away from community education in groups and emphasized the need to maintain physical distancing.









THE QUALITY OF THE RESEARCH meant that they felt confident enough in the recommendations to copy the guidelines straight into a handbook for the ASHAs. This was distributed widely by state governments alongside PPE and training.
Julia Dkhar, a 38-year-old ASHA working in Meghalaya, a state in northeastern India, said that the training, guidelines and equipment were invaluable for her work during the pandemic. At the time, she was visiting around 25 households and speaking to around 60 people a day.

She also knew how to correct the myths and misinformation she heard, including that mosquitoes caused COVID-19, and that people could protect themselves from catching the virus by drinking alcohol and eating garlic.
“Our work actually contributed to preventing and educating and creating that awareness, especially among frontline health workers, and stopping the disease spread,” said Moola.
The team saw recommendations based on their work being adopted nationwide, particularly in Odisha state, which was praised for its response to COVID-19.
After the reports were made public, the researchers got requests through social media to discuss their findings, and the recommendations were also shared by civil society, included in a government app and referenced in World Health Organization interim guidelines on community-based care as well as in a document on preventing violence against women.
THE QUALITY OF THE RESEARCH meant that they felt confident enough in the recommendations to copy the guidelines straight into a handbook for the ASHAs. This was distributed widely by state governments alongside PPE and training.
Julia Dkhar, a 38-year-old ASHA working in Meghalaya, a state in northeastern India, said that the training, guidelines and equipment were invaluable for her work during the pandemic. At the time, she was visiting around 25 households and speaking to around 60 people a day.
She also knew how to correct the myths and misinformation she heard, including that mosquitoes caused COVID-19, and that people could protect themselves from catching the virus by drinking alcohol and eating garlic.
“Our work actually contributed to preventing and educating and creating that awareness, especially among frontline health workers, and stopping the disease spread,” said Moola.
The team saw recommendations based on their work being adopted nationwide, particularly in Odisha state, which was praised for its response to COVID-19.
After the reports were made public, the researchers got requests through social media to discuss their findings, and the recommendations were also shared by civil society, included in a government app and referenced in World Health Organization interim guidelines on community-based care as well as in a document on preventing violence against women.
THE SUCCESS OF THIS REPORT will contribute to more evidence-informed policy-making for health systems in the future.
“In India, getting evidence into policy-making is a priority,” said Ved.
Without it, policy-makers risk making ill-informed, poorly-timed decisions that, in a highly populated and already vulnerable country like India, could cost dearly.
“The implications of that can be quite enormous”.
LOOKING FORWARD

HAVING THE ERA PROJECT UP and running when the unexpected arose meant that the health systems in India and Georgia were better equipped to endure the challenges of COVID-19. They had the tools in place to put evidence-based policy-making at the heart of their response and, as a result, saved lives.
In India and Georgia, the pandemic showed decision-makers, from the highest-offices of power to the front lines of public health, what embedded research can do. Instead of making major decisions based upon intuition or ideology alone, they were able to rely on the most up-to-date evidence to inform their choices and bring evidence-based decision making to the heart of health care policy.
Produced for the Alliance by Fat Rat Films
Acknowledgements
We would like to thank the researchers, policy-makers and ASHAs who gave us their time and told us their stories, even if we couldn’t include them all. In particular for the India story Dr Rajani R. Ved of the National Health Systems Resource Centre, Dr Soumyadeep Bhaumik, Misimi Kakoti, Dr Jyoti Tyagi and Dr Sandeep Moola of The George Institute for Global Health and Julia Dkhar, an ASHA working in Meghalaya. For the Georgia story we would like to thank Dr George Gotsadze, Dr Ivdity Chikovani, Maia Uchaneishvili and Lela Sulaberidze of Curatio International Foundation and Dr Tamar Gabunia of Georgia’s MoILHSA.
This story was created and produced by Fat Rat Films. It was directed by Fred Grace, who also managed the project. It was produced and developed for the web by Jodie Taylor, written by Hannah McNeish, designed by Ian Dutnall. The videos were edited by William Bloomfield, animated by Flavio Fernandini, sound was designed and mixed by Jonathan Tarfur. Meg Amos was assistant producer.
The project was overseen by Jeffrey Knezovich at the Alliance for Health Policy and Systems Research, WHO, who also provided technical and editorial input. The guidance of Dr Abdul Ghaffar and Dr Robert Martin at the Alliance for Health Policy and Systems Research has also been invaluable.
The Alliance is able to conduct its work thanks to the commitment and support from a variety of funders. These include our long-term core contributors from national governments and international institutions, as well as designated funding for specific projects within our current priorities. For the full list of Alliance donors, please visit: https://www.who.int/alliance-hpsr/partners/en/.
Image Credits
ASHA with phone sitting on floor with mother and child
Photographer: Dimagi, Inc.
Video clips from "ASHA - Bringing diabetes care to rural India”
Filmographer: Keld von Eyben | EybenFilm
Project Manager: Brit Susan Larsen | Novo Nordisk
Rapid research responders: The life-saving power of embedded research
ISBN (electronic version)
ISBN (print version)
© World Health Organization 2020
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo.
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. Rapid research responders: The life-saving power of embedded research. Geneva: World Health Organization; 2020.
Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing. Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.